The Crimean-Congo haemorrhagic fever (CCHF) virus causes severe viral haemorrhagic fever outbreaks.
CCHF outbreaks have a case fatality rate of up to 40%.
The virus is primarily transmitted to people from ticks and livestock animals. Human-to-human transmission can occur resulting from close contact with the blood, secretions, organs or other bodily fluids of
infected persons.
CCHF is endemic in Africa, the Balkans, the Middle East and Asia, in countries south of the 50th parallel north.
There is no vaccine available for either people or animals.
Crimean-Congo haemorrhagic fever (CCHF) is a widespread disease caused by a tick-borne virus (Nairovirus) of the Bunyaviridae family. The CCHF virus causes severe viral haemorrhagic fever outbreaks, with a case fatality rate of 10–40%.
CCHF is endemic in Africa, the Balkans, the Middle East and Asian countries south of the 50th parallel north – the geographical limit of the principal tick vector.
The Crimean-Congo haemorrhagic fever virus in animals and ticks
The hosts of the CCHF virus include a wide range of wild and domestic animals such as cattle, sheep and goats. Many birds are resistant to infection, but ostriches are susceptible and may show a high prevalence of infection in endemic areas, where they have been at the origin of human cases. For example, a former outbreak occurred at an ostrich abattoir in South Africa. There is no apparent disease in these animals.
Animals become infected by the bite of infected ticks and the virus remains in their bloodstream for about one week after infection, allowing the tick-animal-tick cycle to continue when another tick bites. Although a number of tick genera are capable of becoming infected with CCHF virus, ticks of the genus Hyalomma are the principal vector.
Transmission
The CCHF virus is transmitted to people either by tick bites or through contact with infected animal blood or tissues during and immediately after slaughter. The majority of cases have occurred in people involved in the livestock industry, such as agricultural workers, slaughterhouse workers and veterinarians.
Human-to-human transmission can occur resulting from close contact with the blood, secretions, organs or other bodily fluids of infected persons. Hospital-acquired infections can also occur due to improper sterilization of medical equipment, reuse of needles and contamination of medical supplies.
Signs and symptoms
The length of the incubation period depends on the mode of acquisition of the virus. Following infection by a tick bite, the incubation period is usually one to three days, with a maximum of nine days. The incubation period following contact with infected blood or tissues is usually five to six days, with a documented maximum of 13 days.
Onset of symptoms is sudden, with fever, myalgia, (muscle ache), dizziness, neck pain and stiffness, backache, headache, sore eyes and photophobia (sensitivity to light). There may be nausea, vomiting, diarrhoea, abdominal pain and sore throat early on, followed by sharp mood swings and confusion. After two to four days, the agitation may be replaced by sleepiness, depression and lassitude, and the abdominal pain may localize to the upper right quadrant, with detectable hepatomegaly (liver enlargement).
Other clinical signs include tachycardia (fast heart rate), lymphadenopathy (enlarged lymph nodes), and a petechial rash (a rash caused by bleeding into the skin) on internal mucosal surfaces, such as in the mouth and throat, and on the skin. The petechiae may give way to larger rashes called ecchymoses, and other haemorrhagic phenomena. There is usually evidence of hepatitis, and severely ill patients may experience rapid kidney deterioration, sudden liver failure or pulmonary failure after the fifth day of illness.
The mortality rate from CCHF is approximately 30%, with death occurring in the second week of illness. In patients who recover, improvement generally begins on the ninth or tenth day after the onset of illness.
Diagnosis
CCHF virus infection can be diagnosed by several different laboratory tests:
enzyme-linked immunosorbent assay (ELISA) ;
antigen detection;
serum neutralization;
reverse transcriptase polymerase chain reaction (RT-PCR) assay; and
virus isolation by cell culture.
Patients with fatal disease, as well as in patients in the first few days of illness, do not usually develop a measurable antibody response and so diagnosis in these individuals is achieved by virus or RNA detection in blood or tissue samples.
Tests on patient samples present an extreme biohazard risk and should only be conducted under maximum biological containment conditions. However, if samples have been inactivated (e.g. with virucides, gamma rays, formaldehyde, heat, etc.), they can be manipulated in a basic biosafety environment.
Treatment
General supportive care with treatment of symptoms is the main approach to managing CCHF in people.
The antiviral drug ribavirin has been used to treat CCHF infection with apparent benefit. Both oral and intravenous formulations seem to be effective.
Prevention and control
Controlling CCHF in animals and ticks
Ticks of the genus Hyalomma are the principal vector of Crimean-Congo haemorrhagic fever (Female is on top and male is below)
Ticks of the genus Hyalomma are the principal vector of Crimean-Congo haemorrhagic fever (Female is on top and male is below)
Robert Swanepoel/NICD South Africa
It is difficult to prevent or control CCHF infection in animals and ticks as the tick-animal-tick cycle usually goes unnoticed and the infection in domestic animals is usually not apparent. Furthermore, the tick vectors are numerous and widespread, so tick control with acaricides (chemicals intended to kill ticks) is only a realistic option for well-managed livestock production facilities.
For example, following an outbreak at an ostrich abattoir in South Africa (noted above), measures were taken to ensure that ostriches remained tick free for 14 days in a quarantine station before slaughter. This decreased the risk for the animal to be infected during its slaughtering and prevented human infection for those in contact with the livestock.
There are no vaccines available for use in animals.
Reducing the risk of infection in people
Although an inactivated, mouse brain-derived vaccine against CCHF has been developed and used on a small scale in eastern Europe, there is currently no safe and effective vaccine widely available for human use.
In the absence of a vaccine, the only way to reduce infection in people is by raising awareness of the risk factors and educating people about the measures they can take to reduce exposure to the virus.
Public health advice should focus on several aspects.
Reducing the risk of tick-to-human transmission:
wear protective clothing (long sleeves, long trousers);
wear light coloured clothing to allow easy detection of ticks on the clothes;
use approved acaricides (chemicals intended to kill ticks) on clothing;
use approved repellent on the skin and clothing;
regularly examine clothing and skin for ticks; if found, remove them safely;
seek to eliminate or control tick infestations on animals or in stables and barns; and
avoid areas where ticks are abundant and seasons when they are most active.
Reducing the risk of animal-to-human transmission:
wear gloves and other protective clothing while handling animals or their tissues in endemic areas, notably during slaughtering, butchering and culling procedures in slaughterhouses or at home;
quarantine animals before they enter slaughterhouses or routinely treat animals with pesticides two weeks prior to slaughter.
Reducing the risk of human-to-human transmission in the community:
avoid close physical contact with CCHF-infected people;
wear gloves and protective equipment when taking care of ill people;
wash hands regularly after caring for or visiting ill people.
Controlling infection in health-care settings
Health-care workers caring for patients with suspected or confirmed CCHF, or handling specimens from them, should implement standard infection control precautions. These include basic hand hygiene, use of personal protective equipment, safe injection practices and safe burial practices.
As a precautionary measure, health-care workers caring for patients immediately outside the CCHF outbreak area should also implement standard infection control precautions.
Samples taken from people with suspected CCHF should be handled by trained staff working in suitably equipped laboratories.
Recommendations for infection control while providing care to patients with suspected or confirmed Crimean-Congo haemorrhagic fever should follow those developed by WHO for Ebola and Marburg haemorrhagic fever.
WHO response
WHO is working with partners to support CCHF surveillance, diagnostic capacity and outbreak response activities in Europe, the Middle East, Asia and Africa.
WHO also provides documentation to help disease investigation and control, and has created an aide–memoire on standard precautions in health care, which is intended to reduce the risk of transmission of bloodborne and other pathogens.
For more information contact:
WHO Media centre















 It is done through a specific bioresonance machine to fully customize this therapy through the combination of energy and electromagnetic waves frequencies appropriate to the individual needs of each patient.
It is done through a specific bioresonance machine to fully customize this therapy through the combination of energy and electromagnetic waves frequencies appropriate to the individual needs of each patient.
 Also check out the
Also check out the 
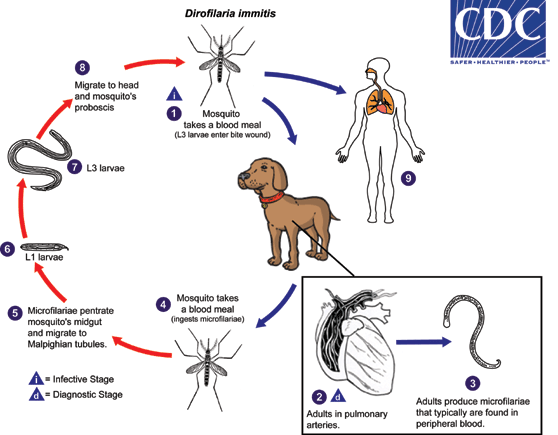
 . In the definitive host, the L3 larvae undergo two more molts into L4 and adults. Adults reside in pulmonary arteries, and are occasionally found in the right ventricle of the heart
. In the definitive host, the L3 larvae undergo two more molts into L4 and adults. Adults reside in pulmonary arteries, and are occasionally found in the right ventricle of the heart  . Adult females are usually 230-310 mm long by 350 µm wide; males are usually 120-190 mm long by 300 µm wide. Adults can live for 5 - 10 years. In the heart, the female worms are capable of producing microfilariae over their lifespan. The microfilariae are found in peripheral blood
. Adult females are usually 230-310 mm long by 350 µm wide; males are usually 120-190 mm long by 300 µm wide. Adults can live for 5 - 10 years. In the heart, the female worms are capable of producing microfilariae over their lifespan. The microfilariae are found in peripheral blood  . A mosquito ingests the microfilariae during a blood meal
. A mosquito ingests the microfilariae during a blood meal  . After ingestion, the microfilariae migrate from the mosquito’s midgut through the hemocoel to the Malpighian tubules in the abdomen
. After ingestion, the microfilariae migrate from the mosquito’s midgut through the hemocoel to the Malpighian tubules in the abdomen  . There the microfilariae develop into first-stage larvae
. There the microfilariae develop into first-stage larvae  and subsequently into third-stage infective larvae
and subsequently into third-stage infective larvae  . The third-stage infective larvae migrate to the mosquito's proboscis
. The third-stage infective larvae migrate to the mosquito's proboscis  and can infect another definitive host when it takes a blood meal
and can infect another definitive host when it takes a blood meal  , D. immitis larvae tend to follow the same migratory pathway as in the canine host, ending up in the lungs, where they often lodge in small-caliber vessels, causing infarcts and typical "coin lesions" visible on radiographs
, D. immitis larvae tend to follow the same migratory pathway as in the canine host, ending up in the lungs, where they often lodge in small-caliber vessels, causing infarcts and typical "coin lesions" visible on radiographs











")














{kind=link}